Masticatory Myositis
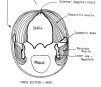
Masticatory mysositis appears to be a breed problem in the Chinese Shar-Pei. While I’m hesitant to say it’s an inherited condition I have seen it in lines and in litters of affected individuals. This condition used to be described as two separate disorders: (1)eosinophilic myositis and (2) atrophic myositis. It is currently felt that these are manifestations of the same disease now called masticatory myositis. This is an inflammatory muscle disease, most likely immune-mediated, involving the muscles of mastication – these muscles are used to grind and chew food prior to swallowing. Five muscle groups in the dog are involved in the process of mastication – four muscles are responsible for closing the mouth and one with opening the mouth. The tempoallis muscles and the masseter muscles are primarily the muscles used to powerfully close the jaws and are espacially well developed in Shar-Pei (Figs. 1 and 2).
| Fig 1 | Fig 2 | Fig 3 |
 |
 |
 |
| Click to Enlarge | Click to Enlarge | Click to Enlarge |
Bear in mind that these muscles must also relax in order for the mouth to open. Since these two muscles are the largest muscles which close the jaw, when they become involved in masticatory myositis, the primary clinical sign is trouble in opening the jaws.
Masticatory myositis can be divided into an acute and chronic form. It must be remembered that one acute attack can lead immediately into the chronic form of the disease, although, more often than not, multiple, recurrent acute attacks are necessary. Symptoms of the acute form involve the the swollen, firm and painful temporalis and masseter muscles. The dog’s head often appears swollen and larger than normal. The dog will be reluctant or unable to open his mouth. Opening the mouth more than 1 inch or so elicits an extremely painful response. This results in difficulty in eating and often the owner notices increased drooling as well. This swelling may even cause exophthalmia or the eyes to “bug out”. Usually a fever is present and the lymph nodes in the head and neck region are enlarged. The tonsils are often enlarged as well, but it is difficult to visualize them due to the inability to open the mouth. The patient is often depressed and may resent palpation of the head musculature.
Laboratory findings are variable, but very often are normal. The white blood cell count may be elevated and often there is an increase in eosinophils (a type of white blood cell often seen with inflammation). Most often there is a dramatic increase in a skeletal muscle enzyme known as creatine kinase or creatine phosphokinase (CPK-MM). Smaller amounts of this enzyme are also located in the brain (CPK-BB) and in the heart muscle (CPK-MB). This enzyme has a short life span in the serum and is most often elevated in the acute form of the disease due to the magnitude of muscle damage and because the owner usually presents the dog while the disease is present. CPK may not be part of the normal serum enzyme panel your veterinarian uses and may have to be requested separately. Your vet should also request the CPK enzyme be reported in terms of the various isoenzymes (heart, brain and skeletal muscles).
The chronic form usually is evident when the dog’s head appears “sunken”, especially the top of the head. Sever and recurrent muscle damage leads to scar tissue formation and atrophy or shrinking of the muscle. This scar tissue is non-functional and these dogs often cannot open their mouths more than 1/2-1 inch. The dog’s head often appears “skull-like” with a prominent external sagittal crest (the bony ridge on top of the head) and the eyes are sometimes enophthalmic or sunken due to loss of the muscle mass behind them (fig.3). In the chronic form, laboratory findings are often normal. The CPK-MM is usually normal due to the fact that there is little muscle left to produce the enzyme. The dogs are normal otherwise and non-painful, although the mouth cannot be opened.
The cause of masticatory myositis is uncertain, but is thought to be immune-mediated because:
- The type of cellular infiltrate in the affected muscles.
- The disease is responsive to immunosuppressive doses of corticosteroids.
- In some cases, autoantibodies are present, fixed to the unique muscles fibers present in the muscles of mastication (Type II M fibers) and the presence of anti-Type II M antibodies in the serum of some dogs with the disease. These antibodies may play a role in the immune system attack on these muscle fibers.
Definitive diagnosis of this condition is based on muscle biopsy — usually of the temporalis and/or masseter muscles. Also a 2M Antibody test is available which can be done utilizing a serum sample — this must be done before therapy is initiated! This test available from:
Basic Science Building, Room 1057
University of California, San Diego
La Jolla, CA 92093-0612
Phone: (858) 534-1537
Fax: (858) 534-7319